
Health
How Pollen Analytics Can Strengthen Nigeria’s Public Health Preparedness
Post Views: 286
The first breath of Harmattan carries more than desert dust. It rolls gently through Lagos in soft, shimmering waves—familiar, almost comforting—until it isn’t. By midday, pharmacies are crowded with people searching for relief from sneezing fits and wheezing chests. Clinics fill with the sound of coughs and shallow breaths. For many, it feels like an annual nuisance that will pass soon enough. But what fills the air is more than dust. Hidden in that golden haze are billions of pollen grains—tiny, invisible particles powerful enough to decide how thousands of Nigerians will breathe, sleep, and live through the season.
For years, we’ve treated these seasonal symptoms as little more than an inconvenience. Yet behind every sneeze and breathless night lies a preventable crisis. Research shows that more than one in four Nigerians now suffer from allergic rhinitis, with cases clustering in cities where pollution and unplanned urban growth trap irritants in the air. The pattern grows clearer each year. Rising temperatures, erratic rainfall, and expanding urban greenery are stretching pollen seasons and introducing new allergens into communities that never experienced them before. The World Health Organization has already warned that warmer climates and higher carbon dioxide levels are creating longer and more intense pollen cycles globally. Nigeria is now feeling that shift in full force.
Across the country, scientists are tracing the evidence. In Abuja, pollen concentrations rise sharply during the late rainy season and Harmattan, when grains released by grasses, weeds, and palm trees fill the air. The TETFund Allergy Project at the University of Lagos has linked these peaks to spikes in asthma, sinus infections, and eye irritation. As pulmonologist Dr Obianuju Ozoh notes, “It is expedient to identify those plants producing airborne pollen allergens for proper diagnosis and treatment.” Without that knowledge, thousands of cases will continue to be misdiagnosed or ignored.
One Lagos study helps show why. In 2015, researchers recorded nearly 3,500 airborne pollen and spore particles in just three months on the University of Lagos campus—mostly from grasses (13.7 percent) and sedges (12.7 percent). They found that rainfall and humidity sharply reduced pollen levels, while drier months triggered dramatic spikes. These findings reveal clear seasonal patterns that could form the backbone of a national forecasting model linking weather conditions to respiratory illness.
Nigeria already has a solid foundation to build on. The Nigerian Meteorological Agency (NiMet) tracks rainfall, temperature, humidity, and wind speed—the same environmental factors that determine how pollen moves across regions. Integrating pollen monitoring into NiMet’s existing weather-station network would require little new infrastructure but could deliver major public-health benefits. With such data, Nigeria could begin tracking invisible health threats alongside traditional weather risks.
Elsewhere, that’s exactly what’s happening. The United States, Japan, and much of Europe run national pollen-monitoring systems that issue daily forecasts similar to weather reports. These alerts help doctors anticipate hospital surges and warn citizens before symptoms appear. Technology companies are joining in: Google’s Pollen API, for instance, uses satellite images and weather data to send hyper-local alerts to users. The goal is simple—to predict allergic reactions before they happen and prevent avoidable suffering.
Imagine Nigeria developing something similar. A digital health-record system could automatically pull in daily pollen and air-quality data. Doctors might notice that a child’s asthma attacks always coincide with high grass-pollen days. Public-health officials could combine this environmental information with medical data to build a National Environmental Health Dashboard—a live map showing respiratory-risk zones across the country. Hospitals could prepare before allergy spikes, communities could plan outdoor events more safely, and health authorities could shift from reacting to preventing.
Such a vision is achievable. During my time leading innovation at the Center for the Prevention of Health Disparities, I helped create a federally supported digital-health project that integrated environmental data into clinical care. Our predictive models could forecast pollen surges up to 72 hours in advance, improving data accuracy by more than 35 percent and cutting processing time by nearly a quarter. We saw firsthand how connecting health-information systems with environmental monitoring gave clinicians and policymakers time to act. Predictive analytics can literally turn air into intelligence—and intelligence into life-saving action.

Nigeria has the right institutions to make this happen. NiMet already collects national climate data. The Nigeria Centre for Disease Control (NCDC) monitors respiratory-disease trends. The Federal Ministry of Health coordinates national surveillance. Universities such as the University of Lagos and Ahmadu Bello University, both home to palynology labs, could serve as scientific partners. Together, they could establish Nigeria’s first National Pollen Monitoring Network, where data from weather stations feed directly into health dashboards, linking environmental triggers to hospital admissions in real time.
There are lessons close to home too. In 2019, South Africa launched a National Pollen Monitoring Network that provides weekly allergy reports from major cities. In the United Kingdom, pharmacists and general practitioners now use pollen forecasts to message high-risk patients before peak exposure. These systems have reduced emergency visits, improved treatment compliance, and raised public awareness. They show what’s possible when environmental data becomes part of national health planning.
For Nigeria, the question isn’t whether such a system can be built—it’s how soon. A modest investment in automated pollen sensors across the six geopolitical zones could transform the nation’s respiratory-health landscape within a few years. Data from NiMet’s stations could feed into NCDC dashboards, made publicly available through real-time pollen maps. Startups and researchers could then use this open data to build local allergy-tracking apps, patient-education tools, and predictive dashboards tailored to Nigeria’s climate. Even a pilot project in Lagos, Abuja, and Kano could generate insights that save lives.
Still, technology alone isn’t enough. Policy and public understanding must grow with innovation. Nigeria’s Ministries of Health, Environment, and Science need to work together to treat environmental data as a core part of preventive medicine. Medical schools should train future clinicians to interpret and use such data. And citizens themselves must be empowered. Imagine receiving a simple text message warning of a high-pollen day—that single alert could prevent an asthma attack, an emergency visit, or even a loss of life.
Having worked on predictive-health systems, I’ve seen how data changes outcomes when paired with human intent. When health agencies combine environmental intelligence with clinical data, they stop reacting to crises and start anticipating them. Patterns that once hid in plain sight suddenly become clear. As Nigeria faces the health impacts of a changing climate, pollen analytics may be one of the most practical and transformative tools available.
Fewer asthma emergencies mean less strain on hospitals, lower costs, and stronger families. But beyond the numbers lies something deeper: empowerment. When people have information, they can protect themselves; when doctors have context, they can diagnose faster; when policymakers have foresight, they can design smarter interventions. The same air that carries risk can also carry resilience—if we choose to measure it.
Pollen counting is more than a scientific exercise. It’s a bridge between environment and health, between what we breathe and how we live. Each grain floating through Nigeria’s skies contains data that could forecast illness, inform care, and ultimately save lives. By embracing pollen analytics, Nigeria can turn an invisible seasonal threat into a visible opportunity for public-health transformation. Counting pollen could quite literally help the nation count healthier tomorrows.
About the author
Obiajuru Triumph Nwadiokwu is a Master of Information Systems Management graduate from Carnegie Mellon University and a Health Information Systems expert. A White House Scholar and Health Analyst Research Associate at the Center for the Prevention of Health Disparities, he has led pioneering research at the intersection of digital health innovation, environmental data, and public health.

Why you feel dizzy when you stand up?
A young, healthy patient asked me: “Doc, sometimes when I stand up from the bed too fast, my vision goes completely black for two seconds and I get dizzy. Am I having a mini-stroke?”
No, it is actually proof that your nervous system is working perfectly.
The exact neurovascular cascade behind why your vision blacks out when you stand up too fast and why you don’t actually pass out. 👇
• The Gravity Drop: When you are lying down, your heart pumps blood easily on a flat plane. The moment you stand up abruptly, gravity instantly pulls about 500 to 800 mL of your blood straight down into your legs.

• The Transient Drain: This sudden pooling means less blood returns to your heart, which temporarily means less blood is pumped up to your head. For a split second, your brain experiences a drop in pressure.
• The Visual Blackout: The retina (the back of your eye) is incredibly sensitive to oxygen and pressure changes. When the blood pressure dips, the retina temporarily shuts down to conserve energy which is exactly why your vision goes black or static.
• The Baroreceptor Rescue: Luckily, you have pressure sensors (baroreceptors) in your neck. Within milliseconds, they detect the blood pressure drop and fire a panic signal to your brainstem.
• The Sympathetic Snap: Your autonomic nervous system instantly kicks in. It violently constricts the blood vessels in your legs and spikes your heart rate, physically squeezing the blood right back up to your brain. Vision restored.
Summary:
First time this happened to me I genuinely thought I was dying.
Turns out my body was just buffering.
Knowing the science changes everything
Here’s what’s actually happening:
When you stand up quickly, gravity pulls blood downward. Your body briefly has less blood reaching the brain. Your nervous system — specifically the baroreceptors –detects this drop and rapidly triggers your heart to beat faster and your blood vessels to constrict, restoring blood flow within seconds.
The momentary blackout and dizziness is just that brief gap before the correction kicks in.
👉Hi, I am Dr. Priyam. I break down complex medical science and advocate for Evidence-Based Medicine. FOLLOW ME for more clinical facts.

can a+ and a+ give birth to o+ or O negative?
Itâs a panic that lands in clinics and WhatsApp groups far too often: âBoth of us are A positive⦠how is our child O negative? Did the lab mess up? Or is something else going on?â
The short, reassuring answer is no lab error, no mystery, and no betrayal. This outcome is completely possible under normal genetics. Hereâs why the âmathâ actually maths perfectly once we look at what blood-type tests really reveal.
Your blood type is decided by two separate systems that most people only see the final phenotype of, not the hidden genes.
ABO system ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸
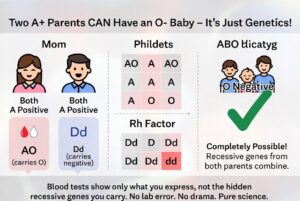
Type A means you carry at least one A allele. You could be AA or AO. The O allele is recessive and invisible in your test result. If both you and your partner are AO (very common), each of you has a 50 % chance of passing the O allele. When both pass O, the child is blood group O. Roughly 45â50 % of people with type A are actually AO carriers, so this pairing happens every day.
Rh (positive/negative) system ð©¸ð©¸ð©¸
âPositiveâ means you have the dominant D antigen. You can still be heterozygous Dd and carry the recessive d allele. If both parents are Dd, there is a 25 % chance the child inherits d from both and is Rh negative. About 15 % of people are Rh negative, which means a large portion of âpositiveâ people quietly carry the d gene.
When both parents are A positive but heterozygous for both traits (AO and Dd), an O-negative child is not only possible â it is mathematically expected in a predictable percentage of pregnancies. The child simply received the two recessive alleles that were hiding in plain sight in both parents.
Blood-group reports show only what antigens are expressed on red cells. They do not sequence your DNA or tell you whether you are homozygous or heterozygous. That hidden information is what allows âimpossibleâ combinations to appear regularly in perfectly ordinary families.
This is basic Mendelian inheritance, not infidelity or laboratory failure. The same recessive-gene logic explains blue-eyed children born to brown-eyed parents or curly-haired kids from straight-haired couples. It is science doing exactly what it is supposed to do.
If the result still feels unsettling, a simple conversation with your doctor or a genetics counsellor can walk you through your specific probabilities. In the overwhelming majority of cases, however, the only thing that needs updating is the outdated assumption that blood types behave like simple labels instead of the elegant, recessive-carrying system they actually are.
Your O-negative child is not evidence of a mistake. They are proof that genetics loves surprises â and that love (and science) are doing just fine.ââââââââââââââââââââââââââââââââââââââââââââââââââ
Dr Parveen Yograj

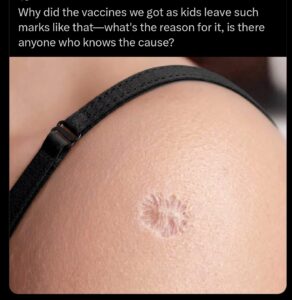
Why does BCG vaccine leave a scar?
That scar on your arm is a battlefield, and the chemistry of how it forms is completely different from any other vaccine you’ve ever received.
Most vaccines inject dead or weakened pathogens into your muscle. Your immune system sees the threat, builds antibodies, done. No lasting damage to the tissue. The BCG tuberculosis vaccine does something radically different. It injects live Mycobacterium bovis bacteria directly into the top layer of your skin, the dermis, and then lets them multiply.
For the first six weeks, those bacteria are actively replicating at the injection site. Your immune system detects them and sends macrophages to engulf the invaders. T-cells get recruited to the area. Then something happens that no other routine vaccine triggers: your body builds granulomas. Those are organized clusters of immune cells that physically wall off the bacteria like a biological quarantine zone. The immune system can’t fully kill every bacterium, so it builds a containment structure around them instead.
That containment war destroys tissue. The granulomas break down the dermis. A blister forms, then an open ulcer that weeps for weeks. The entire process from injection to final scar takes about three months. What you’re left with is the structural aftermath of your immune system demolishing a section of its own skin to contain a live bacterial colony.
The wild part: 4 billion doses administered since 1921. 100 million newborns receive it every year. And the size of your scar correlates with how strong your immune response was. Studies in West Africa found that infants who developed a visible scar had half the mortality rate of infants who didn’t. Not just from TB. From everything. The scar tissue itself became a marker that your immune system trained correctly.
That circular mark is the one vaccine scar that actually means something went right. Your body fought a live infection in a controlled space, won, and left the evidence on your skin for life.
Aakash Gupta

Bauchi man found slaughtered in room as rights group faults police investigation
Liverpool’s Carter Pinnington Set to Join West Brom in Permanent Deal
BREAKING: Amaechi finally agrees to become Atiku’s running mate

Simi Sanya and Femi Dapson Are Now Legally Married and It Is Beautiful to See

FCT Area Council Election: Live results from polling units

Premier League Set-Piece Goals (2025/2026)
-
 Sports1 day ago
Sports1 day agoLewis Hamilton’s Awkward Response to Kimi Antonelli Trolling Kim Kardashian
-
 Sports24 hours ago
Sports24 hours agoFox Break FIFA Broadcasting Rule During Mexico v South Africa
-
 Sports2 days ago
Sports2 days ago‘I’m a 10-Handicap Golfer – Here’s What I Scored Around Shinnecock Ahead of the 2026 US Open’
-
 Sports12 hours ago
Sports12 hours agoReferee Michael Oliver Out of 2026 World Cup Match Due to Injury
-
 Sports13 hours ago
Sports13 hours ago12 Hardest Football Competitions to Win [Ranked]
-
 Sports19 hours ago
Sports19 hours agoEngland Fan Denied World Cup Access After Breaking Trump Rule
-
 Sports2 days ago
Sports2 days agoGary Neville and Roy Keane Slam the US For Banning World Cup Referee
-
 Sports3 hours ago
Sports3 hours ago‘Mistaken Identity’ VAR Check Seen For First Time at 2026 World Cup