
Health
How much does tooth filling cost in Nigeria? (+ Procedures)

How much does tooth filling cost in Nigeria? (+ Procedures), understanding dental filling cost in Nigeria
What you need to know about Tooth Fillings
When one’s tooth is decayed, a dental extraction is not the only solution, as many would erroneously believe. It is now something of a myth that when one has a hole or crack in the tooth and she or she visits a dentist, it is as good as having that tooth removed, which, overtime, has turned out to be as wrong an assertion as any.

A filling is a way to restore a tooth damaged by decay back to its normal function and shape. It is done after the tooth has been assessed by your dentist and he or she sees the need to have the cavity(hole) filled.
First, the teeth surfaces are assessed using a mouth mirror and a dental probe(or explorer). Depending on the extent of the damage on the affected tooth or teeth, he or she may decide to restore the cavity with a filling. Prior to placing a filling, the decayed tooth material is removed and the affected area is cleaned, then restored with a filling material.
By closing off spaces where bacteria can be able to penetrate, a filling also helps prevent further decay.
What are the different types of filling materials?
Materials used for fillings include porcelain, a composite resin (tooth-colored fillings), gold, amalgam (an alloy of metals which include mercury, silver, copper and tin).
The choice of filling materials is dependent on different factors like:
a) The extent of repair necessary.
b) The budget of the patient.
c) History of allergy to certain filling materials.
d) Type of tooth requiring filling(e.g amalgam is used for posterior teeth because of its poor aesthetics).
Amalgam (silver) fillings are resistant to wear and relatively inexpensive. However, due to their dark color, they are more noticeable than porcelain or composite restorations and are not usually used in very visible areas, such as front teeth.
Resins e.g GIC, Composite are tooth coloured and therefore used where aesthetics is of essence, for instance in anterior teeth(incisors and canines). The ingredients are mixed and placed directly into the cavity, where they harden(in some instances with a Curing Lamp). Some resins like Composites may not be the ideal material for large fillings as they may chip or wear over time.
They can also become stained from coffee, tea or tobacco, and do not last as long as other types of fillings.
Porcelain fillings are called inlays or onlays. They are fabricated in a lab and then bonded to the tooth in the dental clinic. They can be matched to the color of the tooth and resist staining. A porcelain restoration generally covers most of the tooth. Their cost is similar to gold.
A tooth filling cannot be done when:
a) there is an extensive decay in a tooth beyond the hard substance(enamel and dentin) into the pulp.
b) a tooth undergoes heavy or abnormal occlusal stress.
c) a tooth is mobile.
d) there are heavy deposits(plaque and calculus) on the tooth surface.
Also, if decay or a fracture has damaged a large portion of the tooth, a crown, or cap, may be required. Decay that has reached the nerve may be treated in two ways: through root canal therapy (in which nerve damaged is removed) or through a procedure called pulp capping/temporary dressing (which attempts to keep the nerve alive).
When the dental filling procedure is complete, it is important for the dentist to spend some time with the patient to discuss how decay can be prevented from forming underneath or near the filling. These methods will also be useful in preventing decay in other teeth.
Patients should be advised to follow good oral care practices, such as brushing their teeth with fluoride toothpaste twice daily, flossing, and using an interdental cleaner daily. Fluoride mouth rinses can also be beneficial for patients with a high risk of further decay.
Follow-up appointments are sometimes required to check the progress of the tooth with the filling and for regular professional cleanings.
How much does tooth filling cost in Nigeria?
The average cost of tooth filling in Nigeria varies across different clinics and it depends on the type of clinic. In private dental clinics, it may cost between N25,000 and N45,000 while in government-owned hospitals, its range is between N10,000 and N20,000. The price of tooth filling in cities like Lagos, Port Harcourt, Enugu, Warri and Abuja may be as high as #60,000 Naira.
Ofonghor Omon (Dental Surgeon)

NSRS CONCLUDES 87TH SCIENTIFIC CONFERENCE IN BENIN, SETS STRATEGIC AGENDA FOR NIGERIA’S SURGICAL WORKFORCE
Benin City, Nigeria — July 2026: The Nigerian Surgical Research Society (NSRS) has successfully concluded its 87th Annual General Meeting and Scientific Conference in Benin City, Edo State, bringing together leading surgeons, researchers, educators, policymakers, and trainees from across the country and beyond.
The conference, hosted at the University of Benin Teaching Hospital (UBTH), focused on one of the most pressing issues in Nigeria’s healthcare sector: the future of the nation’s surgical workforce.
This year’s theme, “Surgical Workforce 2030: Training, Retaining and Task-Sharing in the Nigerian Context,”guided two days of intensive deliberations, scientific presentations, and policy-driven discussions. According to the Chairman of the Local Organizing Committee, Professor Stanley Ukadike Okugbo, the theme “strikes at the very heart of the structural headwinds confronting healthcare delivery in Nigeria today,” highlighting the challenges of brain drain, uneven workforce distribution, and evolving surgical needs.

In his presidential address, Prof. Afeyodion Akhator, President of NSRS, emphasized the urgency of strengthening surgical training programs, improving retention strategies, and adopting safe, evidence-based task-sharing models. He noted that the outcomes of the conference “will influence the direction of surgical education, workforce planning, healthcare policy, and patient care for years to come.”
A major highlight of the event was the keynote lecture delivered by Professor Peter Ndidi Ebeigbe, immediate past President of the National Postgraduate Medical College of Nigeria and Consultant to the World Health
Organization. His address provided a comprehensive roadmap for building a resilient and future-ready surgical workforce, drawing on global best practices and Nigeria’s unique healthcare realities.
The conference featured multiple scientific sessions, exhibitions, debates, and a pre-conference workshop. Delegates presented high-quality abstracts spanning trauma care, oncology, gastrointestinal surgery, surgical
education, and innovations in clinical practice. Participants were also encouraged to experience the cultural richness of Benin City, described in the brochure as “one of Africa’s most historic urban centres and the cradle of the ancient Benin Kingdom.”
The 87th AGM also marked a significant leadership transition for the Society. Members elected a new executive committee to steer NSRS into its next phase of growth, including preparations for the Society’s landmark 50th anniversary in December.

New Executive Committee of the Nigerian Surgical Research Society (NSRS)
• Dr. George C. Obonna — President
• Dr. Clement Odion — Secretary
• Dr. Lucky Ehiagwina — Assistant Secretary
• Dr. Raymond Eghonghon — Treasurer
• Dr. Omorodion Irowa — Auditor
• Prof. Emmanuel Akpo — Editor
• Dr. Francis Campbell — Assistant Editor
• Prof. Aifeyodion Akhator — Ex Officio I
• Prof. Stanley Okugbo — Ex Officio II

Why you feel dizzy when you stand up?
A young, healthy patient asked me: “Doc, sometimes when I stand up from the bed too fast, my vision goes completely black for two seconds and I get dizzy. Am I having a mini-stroke?”
No, it is actually proof that your nervous system is working perfectly.
The exact neurovascular cascade behind why your vision blacks out when you stand up too fast and why you don’t actually pass out. 👇
• The Gravity Drop: When you are lying down, your heart pumps blood easily on a flat plane. The moment you stand up abruptly, gravity instantly pulls about 500 to 800 mL of your blood straight down into your legs.

• The Transient Drain: This sudden pooling means less blood returns to your heart, which temporarily means less blood is pumped up to your head. For a split second, your brain experiences a drop in pressure.
• The Visual Blackout: The retina (the back of your eye) is incredibly sensitive to oxygen and pressure changes. When the blood pressure dips, the retina temporarily shuts down to conserve energy which is exactly why your vision goes black or static.
• The Baroreceptor Rescue: Luckily, you have pressure sensors (baroreceptors) in your neck. Within milliseconds, they detect the blood pressure drop and fire a panic signal to your brainstem.
• The Sympathetic Snap: Your autonomic nervous system instantly kicks in. It violently constricts the blood vessels in your legs and spikes your heart rate, physically squeezing the blood right back up to your brain. Vision restored.
Summary:
First time this happened to me I genuinely thought I was dying.
Turns out my body was just buffering.
Knowing the science changes everything
Here’s what’s actually happening:
When you stand up quickly, gravity pulls blood downward. Your body briefly has less blood reaching the brain. Your nervous system — specifically the baroreceptors –detects this drop and rapidly triggers your heart to beat faster and your blood vessels to constrict, restoring blood flow within seconds.
The momentary blackout and dizziness is just that brief gap before the correction kicks in.
👉Hi, I am Dr. Priyam. I break down complex medical science and advocate for Evidence-Based Medicine. FOLLOW ME for more clinical facts.

can a+ and a+ give birth to o+ or O negative?
Itâs a panic that lands in clinics and WhatsApp groups far too often: âBoth of us are A positive⦠how is our child O negative? Did the lab mess up? Or is something else going on?â
The short, reassuring answer is no lab error, no mystery, and no betrayal. This outcome is completely possible under normal genetics. Hereâs why the âmathâ actually maths perfectly once we look at what blood-type tests really reveal.
Your blood type is decided by two separate systems that most people only see the final phenotype of, not the hidden genes.
ABO system ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸
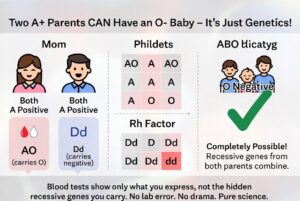
Type A means you carry at least one A allele. You could be AA or AO. The O allele is recessive and invisible in your test result. If both you and your partner are AO (very common), each of you has a 50 % chance of passing the O allele. When both pass O, the child is blood group O. Roughly 45â50 % of people with type A are actually AO carriers, so this pairing happens every day.
Rh (positive/negative) system ð©¸ð©¸ð©¸
âPositiveâ means you have the dominant D antigen. You can still be heterozygous Dd and carry the recessive d allele. If both parents are Dd, there is a 25 % chance the child inherits d from both and is Rh negative. About 15 % of people are Rh negative, which means a large portion of âpositiveâ people quietly carry the d gene.
When both parents are A positive but heterozygous for both traits (AO and Dd), an O-negative child is not only possible â it is mathematically expected in a predictable percentage of pregnancies. The child simply received the two recessive alleles that were hiding in plain sight in both parents.
Blood-group reports show only what antigens are expressed on red cells. They do not sequence your DNA or tell you whether you are homozygous or heterozygous. That hidden information is what allows âimpossibleâ combinations to appear regularly in perfectly ordinary families.
This is basic Mendelian inheritance, not infidelity or laboratory failure. The same recessive-gene logic explains blue-eyed children born to brown-eyed parents or curly-haired kids from straight-haired couples. It is science doing exactly what it is supposed to do.
If the result still feels unsettling, a simple conversation with your doctor or a genetics counsellor can walk you through your specific probabilities. In the overwhelming majority of cases, however, the only thing that needs updating is the outdated assumption that blood types behave like simple labels instead of the elegant, recessive-carrying system they actually are.
Your O-negative child is not evidence of a mistake. They are proof that genetics loves surprises â and that love (and science) are doing just fine.ââââââââââââââââââââââââââââââââââââââââââââââââââ
Dr Parveen Yograj


Tinubu’s choice of Shettima has strengthened APC’s 2027 chances – Ndume
School Abductions: Focus on security, not reelection campaign, Atiku counsels Tinubu
The Ronaldo World Cup 1998 Final ‘Mystery’ that Cost Brazil
Meaning Behind Egypt Manager’s ‘X’ Gesture vs Argentina

Simi Sanya and Femi Dapson Are Now Legally Married and It Is Beautiful to See

Premier League Set-Piece Goals (2025/2026)
-
 Sports1 day ago
Sports1 day agoMbappe’s Brutal Comments About Hakimi After Morocco 0-2 France Go Viral
-
 Sports2 days ago
Sports2 days agoErling Haaland Fumes at World Cup Decision During France vs Morocco
-
 Sports1 day ago
Sports1 day agoSpain’s Luis de la Fuente Issues Strong Verdict on Argentina vs Egypt Referee
-
 Sports1 day ago
Sports1 day agoMichael Olise Stopped From Celebrating France Goal Due to Little-Known Rule
-
 Sports2 days ago
Sports2 days agoWhere Morocco Players Were Born
-
 Sports2 days ago
Sports2 days agoWorld Cup 2026 Goal Songs: Every Team’s Celebration Music
-

 Metro21 hours ago
Metro21 hours agoPolice restrict movement ahead of Edo local government elections
-
 Sports18 hours ago
Sports18 hours agoLineker Brings Up Falklands Ahead of Potential England vs Argentina Tie