
Health
Nigerian Army Medical Test, Screening Tests and Physical Fitness Test

Nigerian Army Medical Test, Screening Tests and Physical Fitness Test.
Thinking about joining the Nigerian Army, Nigerian Navy or the Nigerian Airforce and want to know what happens at the medicals during medical examination including medical tests and physical fitness tests?
The physically and mentally demanding nature of life in the Nigerian Military means there are minimum physical standards that must be met by individuals to ensure the safety of those who join and those who serve alongside them throughout their career.

There are many conditions that can prevent someone from joining the forces, including diabetes or epilepsy which, although are completely manageable on civvy street, could be life-threatening if they were to be deployed somewhere militarily without access to medication.
Therefore, anyone wishing to join the Armed Forces must first undergo and pass a full medical assessment before they can continue with any form of military training.
Medical/Health Questionnaire
All recruits must complete a health questionnaire that asks questions about pre-existing conditions, medication use and surgery history. It is possible at this stage that you may be considered unfit for service or you may experience delays whilst medical records are checked.
Medical Assessment/Medical Examination
All potential recruits must complete the physical medical with a military or MoD approved doctor. The doctor must review and approve your medical history/assessment results before being allowed to progress onto the next stage of Basic Training.
What Is Checked At The Medical Examination?
- Height, weight and BMI
- Lung capacity/peak flow test.
- Blood pressure/pulse.
- Echocardiography
- Chest X-ray
- EEG
- Electrocardiography (electrocardiogram)
- Urine test to check for drugs
- Eyesight and colour perception.
- Audiogram/hearing test (in a soundproof booth).
- Blood tests and screening for HIV, hepatitis B, hepatitis C (this cannot be used to screen you out, just for record purposes)
- Mantoux test for tuberculosis
- Full blood count
- Sickle cell anemia screening
- Exercise spirometry looks at how well your lungs work before and after exercise.
- A physical examination by a doctor will check for hernias/lumps/irregularities.
- Reflexes and joint/muscular movements will also be checked, and recruits will be asked to complete physical movements such as walking on tip toes/heels/press ups and squats.
Hints
_ Avoid loud noise up to 48 hours beforehand.
_ Avoid excessive caffeine consumption. No smoking.
_ Avoid protein drinks.
_Before your medical, it’s important to not have any fizzy drinks, energy drinks, alcohol, or any sugary drinks or foods for at least 12 hours. They can affect your urine sample.
Medical Issues/Problems
Any issues that are flagged up at the medical stage need to be dealt with before continuing with any form of military training.
Certain conditions like asthma can preclude entry to, for example, certain trades in the RAF such as flying branches, but others may require a certain time period to have passed without incident or treatment and subject to a review of medical records before an application will be considered.
Another issue that crops up frequently is past dislocations and surgery on broken bones. It could be that your condition has been misdiagnosed in your notes or it has been misunderstood, for example back pain instead of discomfort or a ligament tear has been interpreted as a dislocation.
If an applicant feels that the decision is wrong they can appeal the decision but they would need to gather as much evidence to support their case as possible which could include further scans/x-rays or a specialist’s opinion. It is also possible that while the Army may reject an application the RAF or Navy may not.
The medical standards do also change over time so what may be a bar to service one year may be considered the following.
Culled from forces.net

Why you feel dizzy when you stand up?
A young, healthy patient asked me: “Doc, sometimes when I stand up from the bed too fast, my vision goes completely black for two seconds and I get dizzy. Am I having a mini-stroke?”
No, it is actually proof that your nervous system is working perfectly.
The exact neurovascular cascade behind why your vision blacks out when you stand up too fast and why you don’t actually pass out. 👇
• The Gravity Drop: When you are lying down, your heart pumps blood easily on a flat plane. The moment you stand up abruptly, gravity instantly pulls about 500 to 800 mL of your blood straight down into your legs.

• The Transient Drain: This sudden pooling means less blood returns to your heart, which temporarily means less blood is pumped up to your head. For a split second, your brain experiences a drop in pressure.
• The Visual Blackout: The retina (the back of your eye) is incredibly sensitive to oxygen and pressure changes. When the blood pressure dips, the retina temporarily shuts down to conserve energy which is exactly why your vision goes black or static.
• The Baroreceptor Rescue: Luckily, you have pressure sensors (baroreceptors) in your neck. Within milliseconds, they detect the blood pressure drop and fire a panic signal to your brainstem.
• The Sympathetic Snap: Your autonomic nervous system instantly kicks in. It violently constricts the blood vessels in your legs and spikes your heart rate, physically squeezing the blood right back up to your brain. Vision restored.
Summary:
First time this happened to me I genuinely thought I was dying.
Turns out my body was just buffering.
Knowing the science changes everything
Here’s what’s actually happening:
When you stand up quickly, gravity pulls blood downward. Your body briefly has less blood reaching the brain. Your nervous system — specifically the baroreceptors –detects this drop and rapidly triggers your heart to beat faster and your blood vessels to constrict, restoring blood flow within seconds.
The momentary blackout and dizziness is just that brief gap before the correction kicks in.
👉Hi, I am Dr. Priyam. I break down complex medical science and advocate for Evidence-Based Medicine. FOLLOW ME for more clinical facts.

can a+ and a+ give birth to o+ or O negative?
Itâs a panic that lands in clinics and WhatsApp groups far too often: âBoth of us are A positive⦠how is our child O negative? Did the lab mess up? Or is something else going on?â
The short, reassuring answer is no lab error, no mystery, and no betrayal. This outcome is completely possible under normal genetics. Hereâs why the âmathâ actually maths perfectly once we look at what blood-type tests really reveal.
Your blood type is decided by two separate systems that most people only see the final phenotype of, not the hidden genes.
ABO system ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸
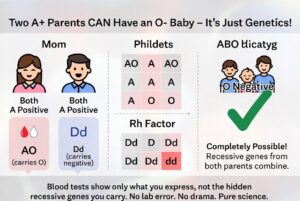
Type A means you carry at least one A allele. You could be AA or AO. The O allele is recessive and invisible in your test result. If both you and your partner are AO (very common), each of you has a 50 % chance of passing the O allele. When both pass O, the child is blood group O. Roughly 45â50 % of people with type A are actually AO carriers, so this pairing happens every day.
Rh (positive/negative) system ð©¸ð©¸ð©¸
âPositiveâ means you have the dominant D antigen. You can still be heterozygous Dd and carry the recessive d allele. If both parents are Dd, there is a 25 % chance the child inherits d from both and is Rh negative. About 15 % of people are Rh negative, which means a large portion of âpositiveâ people quietly carry the d gene.
When both parents are A positive but heterozygous for both traits (AO and Dd), an O-negative child is not only possible â it is mathematically expected in a predictable percentage of pregnancies. The child simply received the two recessive alleles that were hiding in plain sight in both parents.
Blood-group reports show only what antigens are expressed on red cells. They do not sequence your DNA or tell you whether you are homozygous or heterozygous. That hidden information is what allows âimpossibleâ combinations to appear regularly in perfectly ordinary families.
This is basic Mendelian inheritance, not infidelity or laboratory failure. The same recessive-gene logic explains blue-eyed children born to brown-eyed parents or curly-haired kids from straight-haired couples. It is science doing exactly what it is supposed to do.
If the result still feels unsettling, a simple conversation with your doctor or a genetics counsellor can walk you through your specific probabilities. In the overwhelming majority of cases, however, the only thing that needs updating is the outdated assumption that blood types behave like simple labels instead of the elegant, recessive-carrying system they actually are.
Your O-negative child is not evidence of a mistake. They are proof that genetics loves surprises â and that love (and science) are doing just fine.ââââââââââââââââââââââââââââââââââââââââââââââââââ
Dr Parveen Yograj

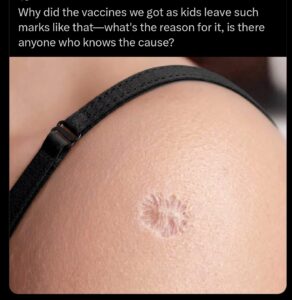
Why does BCG vaccine leave a scar?
That scar on your arm is a battlefield, and the chemistry of how it forms is completely different from any other vaccine you’ve ever received.
Most vaccines inject dead or weakened pathogens into your muscle. Your immune system sees the threat, builds antibodies, done. No lasting damage to the tissue. The BCG tuberculosis vaccine does something radically different. It injects live Mycobacterium bovis bacteria directly into the top layer of your skin, the dermis, and then lets them multiply.
For the first six weeks, those bacteria are actively replicating at the injection site. Your immune system detects them and sends macrophages to engulf the invaders. T-cells get recruited to the area. Then something happens that no other routine vaccine triggers: your body builds granulomas. Those are organized clusters of immune cells that physically wall off the bacteria like a biological quarantine zone. The immune system can’t fully kill every bacterium, so it builds a containment structure around them instead.
That containment war destroys tissue. The granulomas break down the dermis. A blister forms, then an open ulcer that weeps for weeks. The entire process from injection to final scar takes about three months. What you’re left with is the structural aftermath of your immune system demolishing a section of its own skin to contain a live bacterial colony.
The wild part: 4 billion doses administered since 1921. 100 million newborns receive it every year. And the size of your scar correlates with how strong your immune response was. Studies in West Africa found that infants who developed a visible scar had half the mortality rate of infants who didn’t. Not just from TB. From everything. The scar tissue itself became a marker that your immune system trained correctly.
That circular mark is the one vaccine scar that actually means something went right. Your body fought a live infection in a controlled space, won, and left the evidence on your skin for life.
Aakash Gupta

How He Reacted to Red Bull Contract Extension Offer
Food and Drink Prices For England’s 2026 World Cup Match vs Croatia
Thierry Henry’s Viral Analysis on Cristiano Ronaldo For Portugal

Simi Sanya and Femi Dapson Are Now Legally Married and It Is Beautiful to See

FCT Area Council Election: Live results from polling units

Premier League Set-Piece Goals (2025/2026)
-
 Sports13 hours ago
Sports13 hours agoIlia Topuria Said Just 9 Words to His Agent After Justin Gaethje Defeat
-
 Sports1 day ago
Sports1 day agoSaudi Arabia the Only 2026 World Cup Flag That Cannot Touch Ground
-
 Sports15 hours ago
Sports15 hours agoClip of Zinedine Zidane in the Stands During Argentina 3-0 Algeria Goes Viral
-
 Sports2 days ago
Sports2 days agoRodri Labelled ‘Salty’ For Cape Verde Comments After Spain Draw
-
 Sports1 day ago
Sports1 day agoFederico Chiesa U-Turns on Liverpool Exit After Andoni Iraola’s Appointment
-
 Sports1 day ago
Sports1 day agoPetition Demands FIFA Probe into Scotland 1-0 Haiti World Cup Match
-
 Sports1 day ago
Sports1 day ago2 Premier League Clubs Can’t Activate Marcus Rashford’s Release Clause
-
 Sports1 day ago
Sports1 day agoIlia Topuria Said 2 Words to Corner Before Retiring vs Justin Gaethje