
Health
Progress and pain define Nigeria’s cancer response
Post Views: 256
Cancer is quietly becoming Nigeria’s most relentless killer, outpacing a health system still chasing yesterday’s battles.
When the World Health Organization released its new investment case on non-communicable diseases, the findings spoke directly to Nigeria’s unfolding cancer crisis. Globally, cancer and other NCDs claim millions of lives before the age of 70, yet WHO estimates that with just three dollars per person annually, countries could save millions of lives and reap vast economic returns.
For Dr. Nwamaka Lasebikan, former Director of Research and Innovation at the Nigerian Institute for Cancer Research and Treatment (NICRAT), the report reflects realities she encounters every day. “To be honest, the fate of an average Nigerian living with cancer right now is really not too good,” she told healthnews.ng managing editor, Paul Adepoju. “There have been some hitches with the operationalization of the Cancer Health Fund… that disrupted the ability to access funds for the top three cancers — cervical, prostate and breast. So that has impacted negatively really, because as you know, in Nigeria, most patients access their treatment out-of-pocket. And you know what that means in terms of the huge financial burden.”
However, progress has been made in some areas. “In terms of radiotherapy machines, there has been progress,” she explained. “Two months ago, the minister went around to three sites to commission three additional linear accelerators in diverse regions… I think we now have about 16 linear accelerators scattered around the country. We know this is not enough, but I’m highlighting it in the sense of progress.”
Yet diagnostics remain a critical bottleneck. “Survivors actually brought that up,” she said. “They complained that they had to waste resources because tests done in Facility A were not accepted when they went to an oncologist. That begs the question of quality assurance. CT scans are readily available, the problem is affordability. MRIs are not as widely available, and again affordability is the issue. We have only one functional PET scan in Nigeria. These facilities are only in urban settings. In rural settings, they are not there, and women often travel many miles at great cost.”
On financing, she acknowledged new moves but cautioned that the system is still weak. “One of the problems with the Cancer Health Fund was because they wanted to expand the platform to take in more cancers and make funds available to more people. There is also a Catastrophic Health Fund set aside, up to a billion or thereabouts, to cover chronic diseases like kidney disease and cancer. We are expecting a rollout in the not too distant future so patients with cancer can begin to benefit.”
She noted that prevention efforts, particularly on cervical cancer, have gained momentum. “Advocacy is what is driving it,” she said. “The advocacy for cervical cancer elimination is quite high, starting from the WHO asking member states to conform… There was also a time when Nigeria was looking at adopting the WHO plan for breast cancer elimination… but we haven’t heard much about progress yet.”
Health financing models from other countries have struggled to take root. “About four years ago, the ‘sin tax’ was proposed to the National Assembly to increase taxes on sugary beverages and tobacco, but it did not scale because of pushback from those industries,” she recalled. “Other countries like Thailand have had success with such models. Nigeria needs to look at other sources, but as you know, citizens are already struggling with multiple taxes.”

Her deepest concern is not infrastructure but people. “I am exceptionally concerned about the workforce — the dwindling workforce in the oncology space. Not just doctors, but every cadre responsible for delivering safe and effective care. We need to declare a state of emergency. With the trajectory we are on, we will not even be close to meeting the number of oncologists needed in the next 20 to 30 years.”
Still, she finds hope in the growing activism of those who know cancer best. “What I am optimistic about are cancer survivors,” she said. “They are becoming more vocal, demanding a seat at the table, and demanding that their lived experiences are heard. They should be guided so that we can tailor our limited resources for the best gains. We need them to be involved at every level — policy, clinical, and community.”
Her message to Nigerians just beginning the cancer journey is one of caution but also encouragement. “Cancer is not a death sentence,” she said. “We have people who have lived 15 years or more who can speak to that. Alternative practice is becoming common, but while some use it for symptom relief, others abandon treatment for it. I would advise sticking with evidence-based treatments and keeping open communication with doctors. Some complementary medicines can be counterproductive. It is not a sprint, it is a marathon… open communication, early diagnosis, and positivity are key.”
Find below the transcript of Paul’s interview with Dr. Lasebikan.
Q: How would you describe the fate of an average Nigerian living with cancer right now?
A: To be honest, the fate of an average Nigerian living with cancer right now is really not too good. There have been some hitches with the operationalization of the Cancer Health Fund. There was a migration from one platform to the other because we were expecting an expansion of that platform. That disrupted the ability to access funds for the top three cancers — cervix, prostate and breast. So that has impacted negatively really, because as you know, in Nigeria, most patients access their treatment out-of-pocket. And you know what that means in terms of the huge financial burden.
Q: What progress has been made in terms of radiotherapy and diagnostics?
A: In terms of radiotherapy machines, there has been progress. Two months ago, the minister went around to three sites to commission three additional linear accelerators in diverse regions. UNTH already had one radiotherapy machine, then a second one was bought by the federal government. The University of Benin Teaching Hospital had not had a functional radiotherapy facility for many years, so that was also commissioned. There are now about 16 linear accelerators scattered around the country. We know this is not enough, but I’m highlighting it in the sense of progress.
For diagnostics, survivors complained that they had to waste resources because tests done in Facility A were not accepted when they went to an oncologist. That begs the question of quality assurance. CT scans are readily available, the problem is affordability. MRIs are not as widely available, and again affordability is the issue. We have only one functional PET scan in Nigeria. These facilities are only in urban settings. In rural settings, they are not there, and women often travel many miles at great cost.
Q: What about financing cancer treatment?
A: One of the problems with the Cancer Health Fund was because they wanted to expand the platform to take in more cancers and make funds available to more people. There is also a Catastrophic Health Fund set aside, up to a billion or thereabouts, to cover chronic diseases like kidney disease and cancer. We are expecting a rollout in the not too distant future so patients with cancer can begin to benefit.
Q: We hear a lot about cervical cancer elimination. Why is prevention getting more attention there compared to other cancers like breast cancer?
A: Advocacy is what is driving it. The advocacy for cervical cancer elimination is quite high, starting from the WHO asking member states to conform. When we did the cost analysis using the C4-2 costing tool, the amount for prevention of cervical cancer is obviously much less than for tertiary prevention. That point was pushed strongly during the launch. There was also a time when Nigeria was looking at adopting the WHO plan for breast cancer elimination. WHO technical leads are working with NICRAT to see how the global breast cancer initiative can be domesticated, but we haven’t heard much about progress yet.
Q: What about health financing models like taxation on tobacco or sugary drinks, which other countries use?
A: Health financing for cancer requires a lot more development in Nigeria. The Cancer Health Fund was supposed to be co-funded by the private sector, but that has not happened. About four years ago, the “sin tax” was proposed to the National Assembly to increase taxes on sugary beverages and tobacco, but it did not scale because of pushback from those industries. Other countries like Thailand have had success with such models. Nigeria needs to look at other sources, but as you know, citizens are already struggling with multiple taxes.
Q: What are you most concerned about, and what gives you hope?
A: I am exceptionally concerned about the workforce — the dwindling workforce in the oncology space. Not just doctors, but every cadre responsible for delivering safe and effective care. We need to declare a state of emergency. With the trajectory we are on, we will not even be close to meeting the number of oncologists needed in the next 20 to 30 years.
What I am optimistic about are cancer survivors. They are becoming more vocal, demanding a seat at the table, and demanding that their lived experiences are heard. They should be guided so that we can tailor our limited resources for the best gains. We need them to be involved at every level — policy, clinical, and community.
Q: Finally, what would you say to someone just beginning the cancer journey?
A: Cancer is not a death sentence. We have people who have lived 15 years or more who can speak to that. Alternative practice is becoming common, but while some use it for symptom relief, others abandon treatment for it. I would advise sticking with evidence-based treatments and keeping open communication with doctors. Some complementary medicines can be counterproductive with systemic treatments. It is not a sprint, it is a marathon, and many life-changing decisions have to be made. Open communication, early diagnosis, and positivity are key.

NSRS CONCLUDES 87TH SCIENTIFIC CONFERENCE IN BENIN, SETS STRATEGIC AGENDA FOR NIGERIA’S SURGICAL WORKFORCE
Benin City, Nigeria — July 2026: The Nigerian Surgical Research Society (NSRS) has successfully concluded its 87th Annual General Meeting and Scientific Conference in Benin City, Edo State, bringing together leading surgeons, researchers, educators, policymakers, and trainees from across the country and beyond.
The conference, hosted at the University of Benin Teaching Hospital (UBTH), focused on one of the most pressing issues in Nigeria’s healthcare sector: the future of the nation’s surgical workforce.
This year’s theme, “Surgical Workforce 2030: Training, Retaining and Task-Sharing in the Nigerian Context,”guided two days of intensive deliberations, scientific presentations, and policy-driven discussions. According to the Chairman of the Local Organizing Committee, Professor Stanley Ukadike Okugbo, the theme “strikes at the very heart of the structural headwinds confronting healthcare delivery in Nigeria today,” highlighting the challenges of brain drain, uneven workforce distribution, and evolving surgical needs.

In his presidential address, Prof. Afeyodion Akhator, President of NSRS, emphasized the urgency of strengthening surgical training programs, improving retention strategies, and adopting safe, evidence-based task-sharing models. He noted that the outcomes of the conference “will influence the direction of surgical education, workforce planning, healthcare policy, and patient care for years to come.”
A major highlight of the event was the keynote lecture delivered by Professor Peter Ndidi Ebeigbe, immediate past President of the National Postgraduate Medical College of Nigeria and Consultant to the World Health
Organization. His address provided a comprehensive roadmap for building a resilient and future-ready surgical workforce, drawing on global best practices and Nigeria’s unique healthcare realities.
The conference featured multiple scientific sessions, exhibitions, debates, and a pre-conference workshop. Delegates presented high-quality abstracts spanning trauma care, oncology, gastrointestinal surgery, surgical
education, and innovations in clinical practice. Participants were also encouraged to experience the cultural richness of Benin City, described in the brochure as “one of Africa’s most historic urban centres and the cradle of the ancient Benin Kingdom.”
The 87th AGM also marked a significant leadership transition for the Society. Members elected a new executive committee to steer NSRS into its next phase of growth, including preparations for the Society’s landmark 50th anniversary in December.

New Executive Committee of the Nigerian Surgical Research Society (NSRS)
• Dr. George C. Obonna — President
• Dr. Clement Odion — Secretary
• Dr. Lucky Ehiagwina — Assistant Secretary
• Dr. Raymond Eghonghon — Treasurer
• Dr. Omorodion Irowa — Auditor
• Prof. Emmanuel Akpo — Editor
• Dr. Francis Campbell — Assistant Editor
• Prof. Aifeyodion Akhator — Ex Officio I
• Prof. Stanley Okugbo — Ex Officio II

Why you feel dizzy when you stand up?
A young, healthy patient asked me: “Doc, sometimes when I stand up from the bed too fast, my vision goes completely black for two seconds and I get dizzy. Am I having a mini-stroke?”
No, it is actually proof that your nervous system is working perfectly.
The exact neurovascular cascade behind why your vision blacks out when you stand up too fast and why you don’t actually pass out. 👇
• The Gravity Drop: When you are lying down, your heart pumps blood easily on a flat plane. The moment you stand up abruptly, gravity instantly pulls about 500 to 800 mL of your blood straight down into your legs.

• The Transient Drain: This sudden pooling means less blood returns to your heart, which temporarily means less blood is pumped up to your head. For a split second, your brain experiences a drop in pressure.
• The Visual Blackout: The retina (the back of your eye) is incredibly sensitive to oxygen and pressure changes. When the blood pressure dips, the retina temporarily shuts down to conserve energy which is exactly why your vision goes black or static.
• The Baroreceptor Rescue: Luckily, you have pressure sensors (baroreceptors) in your neck. Within milliseconds, they detect the blood pressure drop and fire a panic signal to your brainstem.
• The Sympathetic Snap: Your autonomic nervous system instantly kicks in. It violently constricts the blood vessels in your legs and spikes your heart rate, physically squeezing the blood right back up to your brain. Vision restored.
Summary:
First time this happened to me I genuinely thought I was dying.
Turns out my body was just buffering.
Knowing the science changes everything
Here’s what’s actually happening:
When you stand up quickly, gravity pulls blood downward. Your body briefly has less blood reaching the brain. Your nervous system — specifically the baroreceptors –detects this drop and rapidly triggers your heart to beat faster and your blood vessels to constrict, restoring blood flow within seconds.
The momentary blackout and dizziness is just that brief gap before the correction kicks in.
👉Hi, I am Dr. Priyam. I break down complex medical science and advocate for Evidence-Based Medicine. FOLLOW ME for more clinical facts.

can a+ and a+ give birth to o+ or O negative?
Itâs a panic that lands in clinics and WhatsApp groups far too often: âBoth of us are A positive⦠how is our child O negative? Did the lab mess up? Or is something else going on?â
The short, reassuring answer is no lab error, no mystery, and no betrayal. This outcome is completely possible under normal genetics. Hereâs why the âmathâ actually maths perfectly once we look at what blood-type tests really reveal.
Your blood type is decided by two separate systems that most people only see the final phenotype of, not the hidden genes.
ABO system ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸ð©¸
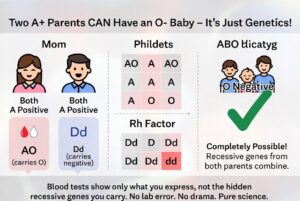
Type A means you carry at least one A allele. You could be AA or AO. The O allele is recessive and invisible in your test result. If both you and your partner are AO (very common), each of you has a 50 % chance of passing the O allele. When both pass O, the child is blood group O. Roughly 45â50 % of people with type A are actually AO carriers, so this pairing happens every day.
Rh (positive/negative) system ð©¸ð©¸ð©¸
âPositiveâ means you have the dominant D antigen. You can still be heterozygous Dd and carry the recessive d allele. If both parents are Dd, there is a 25 % chance the child inherits d from both and is Rh negative. About 15 % of people are Rh negative, which means a large portion of âpositiveâ people quietly carry the d gene.
When both parents are A positive but heterozygous for both traits (AO and Dd), an O-negative child is not only possible â it is mathematically expected in a predictable percentage of pregnancies. The child simply received the two recessive alleles that were hiding in plain sight in both parents.
Blood-group reports show only what antigens are expressed on red cells. They do not sequence your DNA or tell you whether you are homozygous or heterozygous. That hidden information is what allows âimpossibleâ combinations to appear regularly in perfectly ordinary families.
This is basic Mendelian inheritance, not infidelity or laboratory failure. The same recessive-gene logic explains blue-eyed children born to brown-eyed parents or curly-haired kids from straight-haired couples. It is science doing exactly what it is supposed to do.
If the result still feels unsettling, a simple conversation with your doctor or a genetics counsellor can walk you through your specific probabilities. In the overwhelming majority of cases, however, the only thing that needs updating is the outdated assumption that blood types behave like simple labels instead of the elegant, recessive-carrying system they actually are.
Your O-negative child is not evidence of a mistake. They are proof that genetics loves surprises â and that love (and science) are doing just fine.ââââââââââââââââââââââââââââââââââââââââââââââââââ
Dr Parveen Yograj

Date, Nominees & How to Watch 70th Edition Ceremony
Man Utd Now Open Talks To Sign ‘Insane’ Wolves Star
‘Our people interested in choosing leaders’ – Okpebholo commends voters’ turnout in Edo LG election
Meaning Behind Egypt Manager’s ‘X’ Gesture vs Argentina

Simi Sanya and Femi Dapson Are Now Legally Married and It Is Beautiful to See

Premier League Set-Piece Goals (2025/2026)
-
 Sports1 day ago
Sports1 day agoMbappe’s Brutal Comments About Hakimi After Morocco 0-2 France Go Viral
-
 Sports2 days ago
Sports2 days agoErling Haaland Fumes at World Cup Decision During France vs Morocco
-
 Sports1 day ago
Sports1 day agoSpain’s Luis de la Fuente Issues Strong Verdict on Argentina vs Egypt Referee
-
 Sports1 day ago
Sports1 day agoMichael Olise Stopped From Celebrating France Goal Due to Little-Known Rule
-

 Metro1 day ago
Metro1 day agoPolice restrict movement ahead of Edo local government elections
-
 Sports23 hours ago
Sports23 hours agoLineker Brings Up Falklands Ahead of Potential England vs Argentina Tie
-
 Sports8 hours ago
Sports8 hours agoThibaut Courtois Drops Senne Lammens Verdict After World Cup Mistake
-

 Politics23 hours ago
Politics23 hours agoBREAKING: 2027: APC presents Shettima as Tinubu’s running mate